Sickle Cell Disease Treatment in India
Sickle cell disease (SCD) is a genetic blood disorder that affects the shape and function of red blood cells (RBCs), leading to pain, anemia, and potential organ damage. It primarily impacts people from Africa, the Middle East, South Asia, and the Mediterranean region. India is a leading destination for treating sickle cell disease, offering advanced medical care, expert hematologists, and highly affordable treatment options.
The overall cost of Sickle Cell Disease treatment in India ranges from $25,000 to $35,000, which includes standard medical management, medications, diagnostics, supportive care, and a bone marrow transplant (the only potential curative option). This total package cost is significantly lower compared to countries like the USA or the UK, where similar treatment can exceed $200,000 to $300,000. With modern hospitals, personalized protocols, and comprehensive patient support, patients can access life-changing treatment without financial burden.
What Is Sickle Cell Disease?
Sickle cell disease is a hereditary blood disorder that affects hemoglobin within RBCs, the protein responsible for carrying oxygen throughout the body. In people with sickle cell disease, a genetic mutation causes RBCs to become rigid, sticky, and sickle-shaped instead of round and flexible.
These sickle-shaped cells have a shorter lifespan and can block blood flow in vessels, causing pain crises, anemia, and long-term organ damage. SCD is not contagious — it is inherited from parents when a child receives two sickle cell genes. Those with only one sickle gene have “sickle cell trait” and typically show no symptoms.
Globally, SCD is more common in populations of African, Middle Eastern, Indian, and Mediterranean descent. In India, it is more prevalent in tribal populations of Chhattisgarh, Odisha, Maharashtra, Gujarat, and Madhya Pradesh.
What are the Different Types of Sickle Cell Disease?
Sickle cell disease is not a single disorder but a group of inherited conditions that affect hemoglobin. The different types of SCD depend on the combination of abnormal hemoglobin genes a person inherits from their parents.
The main types of sickle cell disease are:
- Hemoglobin SS (Sickle Cell Anemia): It is the most common and severe form of the disease. It develops when a person inherits two sickle cell genes (HbS). People with HbSS often experience frequent pain crises, severe anemia, and a higher risk of complications.
- Hemoglobin SC Disease (HbSC): HbSC occurs when a person inherits one HbS gene and one HbC gene (another abnormal type of hemoglobin). HbSC is generally less severe than HbSS, but it can still cause pain episodes, vision problems, and complications over time.
- Hemoglobin S Beta-Thalassemia (HbS β-thalassemia): It occurs when a person inherits one HbS gene and one beta-thalassemia gene. The severity of symptoms depends on whether the beta-thalassemia gene is mild (β⁺) or severe (β⁰). HbS β⁰-thalassemia can resemble HbSS in severity, while HbS β⁺-thalassemia is often milder.
- Other Rare Types: Rare combinations include HbSD, HbSE, and HbSO-Arab, each caused by the inheritance of HbS with other abnormal hemoglobin variants. These types are uncommon but may still lead to typical sickle cell complications.
What is the Difference Between Sickle Cell Anemia and Sickle Cell Disease?
While often used interchangeably, sickle cell anemia and sickle cell disease are not the same. Understanding the difference between the two diseases is vital for accurate diagnosis and effective treatment planning.
Sickle Cell Disease (SCD)
- Sickle cell disease is the umbrella term that describes a group of genetic blood disorders caused by the presence of abnormal hemoglobin S.
- It includes several genetic variations, such as:
- Hemoglobin SS (Sickle Cell Anemia)
- Hemoglobin SC Disease
- Hemoglobin S Beta-Thalassemia
- And other rarer forms like HbSD, HbSE, and HbSO-Arab
- People with SCD may have different severities and complications depending on the exact genetic type they inherit.
Sickle Cell Anemia (SCA)
- SCA is the most severe and common type of Sickle Cell Disease.
- It specifically refers to individuals with two sickle cell genes (HbSS)—one from each parent.
- Patients with SCA are more likely to experience frequent pain crises, severe anemia, delayed growth, infections, and organ complications.
Sickle Cell Disease Treatment Cost in India
Sickle cell disease (SCD) is a genetic blood disorder that affects the shape and function of red blood cells (RBCs), leading to pain, anemia, and potential organ damage. It primarily impacts people from Africa, the Middle East, South Asia, and the Mediterranean region. India is a leading destination for treating sickle cell disease, offering advanced medical care, expert hematologists, and highly affordable treatment options.
The cost of sickle cell disease treatment in India ranges from $3,000 to $5,000 for standard care and medications, while a bone marrow transplant (the only potential cure) costs between $20,000 and $35,000, which is significantly lower than in countries like the USA or the UK. With modern hospitals, personalized protocols, and comprehensive patient support, India is helping international patients access life-changing treatment without a financial burden.
What are the Common Symptoms and Complications of Sickle Cell Disease?
Sickle cell disease affects every system of the body, primarily because the abnormally shaped red blood cells can't flow smoothly through blood vessels. It causes blockages, low oxygen delivery, and tissue and organ damage. Symptoms can start as early as infancy and tend to vary in severity over time.
The most common symptoms and complications associated with sickle cell disease are:
- Chronic Anemia: Patients with SCD have a constant shortage of healthy red blood cells. It leads to fatigue, paleness, shortness of breath, and delayed growth in children.
- Pain Episodes (Sickle Cell Crises): The hallmark of SCD is periodic severe pain caused by blocked blood flow in bones, joints, chest, or abdomen. These crises may last hours to days and often require hospitalization.
- Swelling of Hands and Feet: Blockages in small blood vessels of the limbs can cause painful swelling, especially in infants and toddlers.
- Frequent Infections: SCD can damage the spleen, making patients more susceptible to bacterial infections, such as pneumonia and meningitis. Preventive antibiotics and vaccinations are essential.
- Vision Problems: Sickle-shaped cells can block tiny vessels in the eyes, leading to retinopathy, blurry vision, or even blindness if untreated.
- Delayed Growth and Puberty: Poor oxygen delivery and chronic anemia can lead to delayed physical and sexual development in children and teens.
- Stroke and Neurological Issues: Children and adults with SCD are at higher risk of stroke, especially if the brain's blood vessels are narrowed or blocked. Regular screenings are crucial for preventing long-term brain damage.
- Acute Chest Syndrome: A life-threatening complication involving chest pain, fever, and breathing difficulty caused by blocked blood vessels in the lungs. Requires immediate medical attention.
- Organ Damage: Over time, SCD can cause damage to organs such as the kidneys, liver, lungs, and heart due to a lack of oxygen and repeated cell damage.
How Is Sickle Cell Disease Diagnosed?
Diagnosing sickle cell disease involves a combination of blood tests that check for abnormal hemoglobin types. In India, both newborn screening programs and diagnostic evaluations for individuals with symptoms are widely available in modern hospitals.
The key diagnostic methods used to confirm sickle cell disease are:
- Hemoglobin Electrophoresis: It is the most reliable test for identifying different types of hemoglobin in the blood. It can confirm the presence of hemoglobin S, C, and beta-thalassemia variants. It is also used to distinguish between Sickle Cell Trait and full-blown Sickle Cell Disease.
- Complete Blood Count (CBC): A CBC helps detect anemia, which is commonly seen in patients with SCD. It measures hemoglobin levels, red blood cell size, and white blood cell count.
- Peripheral Blood Smear: This test involves examining RBCs under a microscope to assess their morphology and characteristics. It helps identify sickle-shaped cells, giving a quick visual confirmation.
- High-Performance Liquid Chromatography (HPLC): HPLC is another accurate method used to quantify different types of hemoglobin. It is widely used in India for both screening and diagnosis.
- Genetic Testing: DNA-based tests can detect mutations in the HBB gene, which is responsible for SCD. It is beneficial for carrier testing, prenatal diagnosis, or confirming rare variants.
- Newborn Screening (NBS): Some Indian states have introduced free newborn screening programs in high-risk areas, particularly among tribal or rural populations. Early diagnosis enables timely vaccination, antibiotic prophylaxis, and effective parental education.
- Imaging and Organ Function Tests: Additional tests, such as transcranial Doppler ultrasound (TCD), echocardiogram, and liver/kidney function tests, are performed to monitor complications.
What are the Treatment Options for Sickle Cell Disease in India?
India offers a wide range of options for the treatment of sickle cell disease, focusing on both symptom management and long-term disease control. While there is no universal cure, many patients can lead healthier lives with proper medical care, and in some cases, a bone marrow transplant (BMT) offers a potential cure.
Below are the primary treatment options available in India:
- Medications to Manage Symptoms: Hydroxyurea is widely used in India to reduce the frequency of painful crises and reduce the need for blood transfusions. Folic acid supplements aid in the production of red blood cells. Pain relief medications such as NSAIDs are used during acute episodes. Doctors prescribe antibiotics (like penicillin) to prevent infections, especially in young children.
- Blood Transfusions: Used to treat severe anemia or complications like stroke or acute chest syndrome. Exchange transfusions are also available in advanced centers for patients with recurring complications. Hospitals in India adhere to stringent blood safety protocols to prevent infections and adverse reactions.
- Iron Chelation Therapy: For patients receiving frequent transfusions, iron overload can occur. Oral chelating agents, such as deferasirox, are used to remove excess iron from the body.
- Vaccination and Infection Prevention: Patients are given vaccines for pneumococcus, meningococcus, and Haemophilus influenzae to prevent severe infections. Indian hospitals ensure that immunization schedules are followed strictly, especially in pediatric patients.
- Bone Marrow or Stem Cell Transplant (Curative Option): BMT is the only potential cure for sickle cell disease. It replaces the patient's defective bone marrow with healthy donor stem cells.
- Counseling and Genetic Education: Genetic counseling is available to help families understand inheritance patterns and risks to future children. Carriers (with Sickle Cell Trait) are also advised on reproductive options.
- Lifestyle and Dietary Management: Patients are guided to maintain hydration, avoid high altitudes or extreme temperatures, and follow a nutritious diet rich in iron and vitamins.
Managing Sickle Cell Crises and Pain Episodes
One of the most distressing aspects of sickle cell disease is the unpredictable and intense pain episodes, commonly known as sickle cell crises. The blockage of blood flow causes these episodes due to the agglutination of sickle-shaped red blood cells in the blood vessels.
In India, hospitals use a stepwise and personalized approach to manage these painful events and reduce their frequency and severity.
- Pain Management Protocols: Mild to moderate pain is typically treated with oral medications, such as paracetamol or ibuprofen. For severe pain, intravenous opioids (e.g., morphine) may be used under close monitoring. Pain assessments are conducted regularly, and dosing is adjusted based on the patient's response.
- Intravenous Fluids and Hydration: Patients are administered IV fluids to help dilute the blood and improve circulation, reducing the severity of a crisis. Oral rehydration is also emphasized in mild cases to prevent dehydration-related triggers.
- Oxygen Therapy: Supplemental oxygen is administered when signs of respiratory distress or low oxygen saturation levels are present during a crisis. It helps maintain tissue oxygenation and reduces further sickling of cells.
- Treating Underlying Triggers: Infections, cold weather, dehydration, stress, and high altitudes are common triggers of pain crises. Indian hospitals work to quickly identify and treat the root cause, such as initiating antibiotics for infection or adjusting medications.
- Preventive Measures: Patients are educated on how to avoid known triggers, including staying hydrated, avoiding strenuous exercise, and protecting against cold exposure. Hydroxyurea is prescribed to reduce the frequency of crises in eligible patients.
Bone Marrow Transplant for Sickle Cell Disease
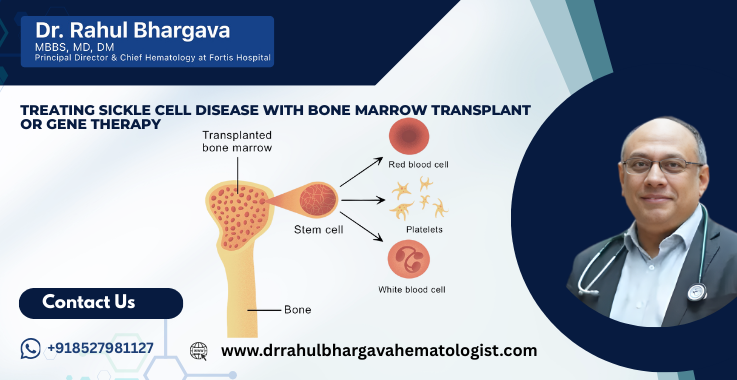
A bone marrow transplant (BMT), also known as a stem cell transplant, is currently the only curative treatment available for sickle cell disease. It works by replacing the patient's defective bone marrow, where sickled red blood cells are produced, with healthy stem cells from a donor. In India, this procedure is becoming increasingly accessible and is performed according to international standard protocols at an affordable cost.
How Does the Transplant Work?
- The patient undergoes conditioning therapy (chemotherapy) to destroy the diseased marrow.
- Healthy hematopoietic stem cells are then infused from a matched donor, usually a fully HLA-matched sibling.
- The donor cells travel to the marrow and start producing normal red blood cells without the sickle shape.
Who Is Eligible for a Bone Marrow Transplant?
- Ideal candidates include:
- Children or young adults with severe SCD and a history of complications.
- Patients with frequent pain crises, stroke, or organ damage.
- Those with an HLA-matched sibling (a perfect genetic match).
- Recent advances have also made it possible to consider haploidentical (half-matched) transplants when full matches are not available.
- Hospitals use advanced HLA typing technology to find compatible family donors.
- Unrelated donor registries and haploidentical (from a parent or sibling) transplants are also being increasingly used.
What is the Cost of Sickle Cell Disease Treatment in India?
India is one of the most cost-effective destinations for Sickle Cell Disease treatment. The overall treatment cost ranges between $25,000 and $35,000, depending on the hospital, donor availability, and patient condition.
This total cost generally includes:
Outpatient management
Diagnostic tests
Medications
Blood transfusions (if needed)
Iron chelation (if needed)
Pediatric care (if applicable)
Bone marrow transplant procedure
ICU & hospitalization
Donor evaluation & stem cell harvest
Post-transplant follow-up & medications
No separate small costs are shown because the care is commonly provided as a complete package for international patients.
What are the Factors Influencing the Cost of Sickle Cell Disease Treatment in India?
The cost of treating sickle cell disease in India can vary from patient to patient, depending on several medical and logistical factors. Below are the key factors that influence the overall cost:
- Type and Severity of the Disease: Patients with sickle cell anemia (HbSS) or severe complications like stroke, frequent crises, or acute chest syndrome often require intensive and prolonged treatment, raising overall costs. Milder forms, such as HbSC, may require only basic medical management.
- Treatment Approach Chosen: Standard care, including medications and transfusions, is less expensive than advanced interventions. A bone marrow transplant significantly increases upfront costs due to hospitalization, conditioning therapy, and monitoring.
- Donor Availability for Bone Marrow Transplant: A fully matched sibling donor reduces cost and complexity. If a haploidentical (half-matched) or unrelated donor is used, costs increase due to the need for specialized protocols and higher risk management for GVHD.
- Choice of Hospital and City: Top-tier private hospitals in metros like Delhi, Mumbai, and Bangalore may charge more than mid-tier centers in smaller cities. However, premium hospitals also offer world-class infrastructure, multilingual staff, and comprehensive international patient services.
- Length of Hospital Stay: Complications such as infections, organ involvement, or transplant-related issues may lead to longer inpatient stays, especially in BMT patients. ICU admissions or isolation rooms add to the cost.
- Post-Treatment Care and Follow-Up: Long-term monitoring, medication, and lab tests after a transplant or frequent crises contribute to ongoing costs. Teleconsultations and remote follow-ups are often available for international patients, minimizing travel costs.
- Age and Overall Health of the Patient: Pediatric patients or those with multiple organ issues may require specialized care, nutritional support, and pediatric ICU backup, influencing cost. Pre-existing conditions can complicate treatment, necessitating additional diagnostic tests or therapies to address the underlying issues.
- Accommodation and Travel Logistics: Although not directly medical, lodging, food, interpreter services, and transportation significantly impact the total treatment budget for international patients and their families.
Cost Comparison: India vs. Other Countries
One of the most significant advantages of seeking Sickle Cell Disease (SCD) treatment in India is the considerable cost savings without compromising on the quality of care. Indian hospitals offer globally recognized expertise, modern technology, and specialized treatment protocols at a fraction of the cost compared to Western nations.
Bone Marrow Transplant
|
Country |
Estimated Cost (USD) |
Notes |
|
India |
$25,000 – $35,000 |
Includes hospital stay, pre- and post-transplant care, and medications |
|
United States |
$200,000 – $300,000 |
Excludes long-term follow-up and may vary by insurance coverage |
|
United Kingdom |
$150,000 – $250,000 |
Covered by the NHS in rare cases, but long wait times are possible |
|
Turkey |
$40,000 – $60,000 |
Costs lower than the West but still significantly higher than India |
Outpatient Management (Medications, Transfusions, etc.)
|
Country |
Annual Cost Estimate (USD) |
Includes |
|
India |
$1,200 – $3,500 |
Medications, transfusions, and doctor visits |
|
USA/UK |
$10,000 – $25,000 |
Costs can be higher without insurance |
|
Gulf Countries |
$8,000 – $20,000 |
Insurance-dependent; limited curative options |
|
South Africa |
$5,000 – $10,000 |
Government hospitals are available, but with limited capacity |
Pediatric Sickle Cell Care in India
Children with Sickle cell disease require specialized, age-appropriate care to manage symptoms, prevent complications, and support their overall development. India is home to several pediatric centers and hematology units that provide comprehensive care tailored for young patients, often at much lower costs than in Western countries.
- Early Diagnosis and Screening: Many Indian hospitals now conduct newborn screening programs to detect SCD early, especially in high-risk tribal and rural populations. Early detection allows timely intervention with antibiotics, vaccines, and parental education.
- Routine Monitoring and Preventive Care: Pediatric SCD patients are monitored for growth delays, developmental milestones, and organ health. Doctors ensure timely vaccination against pneumococcus, meningococcus, and influenza to prevent life-threatening infections. Prophylactic antibiotics, such as penicillin, are typically administered until at least age 5.
- Management of Pain and Crises in Children: Indian pediatricians follow the WHO guidelines for pain control, adjusting dosages according to age and weight. Child-friendly environments and psychological support help manage anxiety and discomfort during hospital visits.
- Nutritional Support: Pediatric nutritionists ensure that children receive a well-balanced diet (rich in iron, folic acid, and vitamins) to promote healthy red blood cell production and immune function. Supplements are provided when needed.
- Education and Family Counseling: Parents are trained to identify early signs of complications, manage fever or pain at home, and ensure medication compliance. Genetic counseling is offered to families with more than one affected child or carrier.
- Pediatric Bone Marrow Transplant Services: India offers child-focused transplant units with pediatric ICU, isolation rooms, and post-transplant care for children undergoing curative treatment. BMT in younger patients has a higher success rate, especially when done early.
Stem Cell Transplant Protocols and Recovery Timeline
Hematopoietic stem cell transplant, or HSCT, is the only curative treatment for sickle cell disease. In India, this advanced procedure is carried out under strict international protocols to ensure safety, efficacy, and long-term success.
- Pre-Transplant Evaluation and Matching: The patient undergoes a thorough medical workup, including imaging studies, blood tests, and assessments of organ function. HLA typing is performed to identify a suitable donor, typically a matched sibling or a half-matched family member (haploidentical). Psychological counseling and financial planning are also part of this phase.
- Conditioning Regimen (Preparation Phase): The patient receives low-dose or myeloablative chemotherapy to destroy the defective bone marrow. This phase typically lasts 5–7 days and prepares the body to accept the donor's healthy stem cells.
- Stem Cell Infusion (Transplant Day): On transplant day (commonly referred to as Day 0), healthy stem cells are infused into the bloodstream. It is a painless, non-surgical procedure similar to a blood transfusion.
- Engraftment and Recovery: Engraftment refers to the stage when donor stem cells start producing new, healthy blood cells. It usually occurs within 2–3 weeks post-transplant. Patients are closely monitored for signs of infection, organ function, and graft-versus-host disease (GVHD).
- Hospital Stay Duration: The inpatient hospital stay typically lasts 5 to 7 weeks, depending on the patient's response. Patients are cared for in sterile transplant units with strict infection control.
- Post-Transplant Follow-Up Timeline: The first 100 days post-transplant are the most critical. Patients attend frequent check-ups for blood counts, immune recovery, organ monitoring, and infection surveillance. After 6 months, visits reduce in frequency, and by 1 year, most patients can resume normal activities if recovery is smooth.
- Return to Normal Life: Children often resume school within 6–9 months. Adults may return to work and daily activities within 9 to 12 months, depending on the pace of their recovery.
Success Rates of Bone Marrow Transplant for Sickle Cell Disease
Bone marrow transplant is a life-changing procedure for eligible patients with sickle cell disease, and success rates in India are now comparable to global standards. With improved donor matching techniques, supportive care, and experienced transplant teams, India offers a high chance of a cure, especially in children and young adults.
Average Success Rate in India
- Patients who undergo successful transplants in India often achieve normal hemoglobin levels, are free from pain crises, and no longer need transfusions or medications. Studies show that 90% of such patients enjoy a normal life expectancy with good quality of life.
- The success rate for matched sibling donor transplants in India ranges from 85% to 92%, particularly when performed in experienced centers.
- For haploidentical (half-matched) transplants, success rates range between 70% and 80%, depending on the patient's health and donor compatibility.
Key Factors That Influence Success
- Early transplantation, especially in children before severe complications set in, leads to better outcomes.
- The availability of a fully HLA-matched sibling donor significantly improves the chances of engraftment and survival.
- Transplants done in JCI-accredited or NABH-certified Indian hospitals ensure adherence to international standards.
- Proper pre-transplant conditioning and post-transplant care reduce the risks of rejection or complications.
- Indian hospitals have made advancements in GVHD prevention protocols through precise donor matching and immune suppression techniques. The incidence of severe GVHD has dropped considerably, enhancing both short- and long-term transplant success.
Life Expectancy and Long-Term Outlook for Sickle Cell Patients
The life expectancy and long-term outlook for individuals with sickle cell disease have improved significantly over the past few years. With the proper medical care, many patients can now lead long, productive, and pain-free lives.
Life Expectancy with Standard Treatment
- Without curative treatment, life expectancy for SCD patients traditionally ranged between 40 to 60 years, depending on access to care and complications.
- In India, with improved access to hydroxyurea, antibiotics, and transfusion services, patients are living well into their 50s and 60s, even without a transplant.
- Lifelong management of infections, pain crises, and organ health is key to maintaining stability.
Life Expectancy After Bone Marrow Transplant
- For patients who undergo a successful bone marrow or stem cell transplant, life expectancy is close to that of a healthy individual.
- Such patients no longer experience sickle cell crises or require chronic medications.
- Studies show that more than 90% of transplant survivors live healthy lives beyond 10–15 years post-transplant.
Patient Testimonials
Here are some real-life experiences of international and Indian patients who underwent successful treatment for sickle cell disease in India. These stories highlight not just the clinical success but also the compassionate care and cost-effective treatment that India is known for.
Mekdes T., Ethiopia – Bone Marrow Transplant for Teenage Daughter
"My daughter suffered from painful crises almost every month. Doctors in Ethiopia said a transplant was the only cure, but we couldn't afford it locally. We came to India after contacting a hospital recommended by friends. The transplant was successful, and the care we received was beyond our expectations. Now she's healthy, and we are so relieved as parents."
Kwame B., Ghana – Comprehensive SCD Care at Affordable Cost
"Living with SCD meant constant pain and missing school for my son. India offered both quality and affordability. We received expert care and detailed explanations from the doctors. The medical staff were kind, and the cost was very reasonable compared to what we were quoted in Europe. We felt supported every step of the way."
Sara M., Iran – Successful Treatment and Excellent Follow-Up
"My brother had frequent complications, and we were afraid of long-term damage. We heard about successful bone marrow transplants in India and decided to give it a try. The doctors were experienced, and they followed international protocols. Even after we returned to Iran, they continued to stay in touch for follow-up. We are delighted and thankful."
Yousef A., Libya – Expert Doctors and Smooth Visa Process
"Finding affordable and advanced treatment for sickle cell in Libya was very hard. In India, we not only found experienced doctors but also a hospital that helped us with the entire travel and visa process. My child has not had a crisis since the transplant, and I am confident we made the best decision for his future."
Conclusion
India is one of the safest, most advanced, and most affordable centers for sickle cell treatment and bone marrow transplant. With a total treatment package costing $25,000 to $35,000, patients can access world-class care, international protocols, and successful outcomes at a fraction of Western costs.
Frequently Asked Questions
Yes, sickle cell disease can be cured in India through a bone marrow or stem cell transplant. This curative treatment is widely available in top hospitals across India and offers high success rates, primarily when performed at a younger age with a suitable donor.
The cost of managing sickle cell disease with medications, regular check-ups, and supportive care ranges from $3,000 to $6,500 annually. For patients undergoing a bone marrow transplant, the total cost typically ranges from $20,000 to $35,000, depending on the hospital, the type of donor, and the length of hospital stay.
Yes, Indian hospitals are globally recognized for their safety, infrastructure, and medical excellence. Most leading centers are NABH or JCI-accredited and follow international protocols. They also have dedicated international patient coordinators to assist with logistics, treatment planning, and aftercare.
To start sickle cell disease treatment in India, international patients must provide copies of their passports, recent medical records, diagnostic test results, and a physician's note, if available. A valid medical visa is also required, and hospitals typically assist patients in obtaining one by issuing a visa invitation letter.
Patients undergoing a bone marrow transplant typically stay in India for six to eight weeks, covering pre-transplant evaluation, the procedure, and recovery. Those seeking medical management or diagnosis alone can expect a stay of one to two weeks, depending on their condition.
Yes, many Indian hospitals specialize in pediatric bone marrow transplants. Children often show better outcomes due to their resilience and fewer existing complications.
The success rate for bone marrow transplants using fully matched sibling donors ranges from 85% to 92%. For half-matched or unrelated donors, the success rate is approximately 70% to 80%, depending on the hospital's experience and the patient's overall health condition.
Yes, most reputed hospitals in India offer interpretation services for international patients. Language support is available in Arabic, French, Amharic, Swahili, and several other languages, ensuring clear communication during the treatment journey.
When a fully matched sibling donor is not available, Indian doctors explore other options, such as haploidentical (half-matched) or unrelated donor transplants. These procedures are now routinely performed in India with high safety and success rates.
Yes, Indian hospitals provide remote follow-up through telemedicine. Patients can consult their doctors via video calls or email, share lab results, and receive guidance on medications and recovery from the comfort of their home country.